

深部侵袭性血管黏液瘤(deep aggressive angiomyxoma,DAA)是一种罕见的间叶黏液样肿瘤,好发于中青年女性的骨盆部位的软组织,如会阴及阴道壁[1]。由于该病的发病率较低,病因、诊断和治疗尚不明确。现报告济宁市第一人民医院(我院)妇科收治的1例高龄女性盆腔DAA的诊治经过,以期为临床诊疗提供思路。
1 病例报告
患者 女,86岁,因发现盆腔肿物4年余、左下腹间断性疼痛1年,于2024年8月8日就诊于我院妇科门诊。患者曾于2019年5月14日因宫颈肌瘤于我院行经腹全子宫切除术+双侧附件切除术,术后半年于我院妇科门诊复查妇科彩色多普勒超声提示盆腔内混合回声团块,大小约8.2 cm×8.6 cm×8.6 cm,考虑患者高龄,嘱暂观察,择期复查,若有不适及时处理。术后半年至今定期复查彩色多普勒超声均提示盆腔肿物持续存在,未予特殊处理。近1年出现左下腹间断性疼痛,2024年7月4日于外院门诊行妇科彩色多普勒超声示:盆腔内探及大小约9.3 cm×11.3 cm×10.2 cm团块样回声,内可见血流信号。患者为求进一步诊治就诊于我院妇科门诊,遂于2024年8月15日以“盆腔肿物,子宫及双侧附件切除术后”收入院。
入院查体:外阴发育正常,阴道通畅,阴道残端愈合良好,盆腔内扪及肿物,大小约10 cm,活动度一般,无明显压痛。完善术前相关辅助检查,2024年8月15日查血常规示:平均血小板体积8.30 fL(参考值:9.2~12 fL),血小板分布宽度8.50 fL(参考值:9.6~15.2 fL),大型血小板比例11.4%(参考值:19.7%~42.4%)。D-二聚体1.11 mg/L(参考值:0~0.5 mg/L)。肝功能检查示:三酰甘油2.01 mmol/L(参考值:0~1.7 mmol/L),高密度脂蛋白胆固醇1.61 mmol/L(参考值:1.29~1.55 mmol/L),低密度脂蛋白胆固醇4.76 mmol/L(参考值:0~3.37 mmol/L),极低密度脂蛋白胆固醇0.91 mmol/L(参考值:0~0.78 mmol/L),脂蛋白a 0.35 g/L(参考值:0~0.3 g/L)。肿瘤标志物检查示:糖类抗原125(carbohydrate antigen 125,CA125)、CA19-9、癌胚抗原(carcinoembryonic antigen,CEA)、鳞状细胞癌抗原(squamous cell carcinoma antigen,SCCA)、甲胎蛋白(alpha-fetoprotein,AFP)及人附睾蛋白4(human epididymis protein 4,HE4)均未见异常。盆腔磁共振成像(magnetic resonance imaging,MRI)示:子宫及双侧附件切除术后;盆腔内见团块状混杂信号影,病灶边界清,边缘规整,大小约12.2 cm×10.4 cm×9.6 cm,T1加权成像(T1 weighted imaging,T1WI)以低、等信号为主,T2WI以高信号为主,弥散加权成像(diffusion weighted imaging,DWI)局部呈高信号(见图1)。2024年8月17日全腹CT示:盆腔巨大软组织肿块影,密度不均,局部可见结节状钙化影,增强扫描呈不均匀强化。考虑患者高龄,遂于2024年8月22日行超声引导下盆腔肿物穿刺活检术,术后病理回报:梭形细胞肉瘤。免疫组织化学检查示:结蛋白(Desmin,+),高分子量钙调蛋白结合蛋白(H-Caldesmon,-),CD34(-),CD117(-),Dog-1(-),细胞角蛋白(Cytokeratin,CK,-),S-100(-),抑制素-a(Inhibin-a,-),CD10(-),周期蛋白D1(Cyclin D1,-),B细胞淋巴瘤-2(B-cell lymphoma 2,Bcl-2,部分+),平滑肌肌动蛋白(smooth muscle actin,SMA,-),肾母细胞瘤基因1(Wilms tumor gene 1,WT1,-),间变性淋巴瘤激酶(anaplastic lymphoma kinase,ALK,-),成肌分化因子1(myogenic differentiation 1,MyoD1,部分+),Ki-67增殖指数(约3%+)。病理结合免疫组织化学结果,考虑为梭形细胞横纹肌肉瘤。
图1
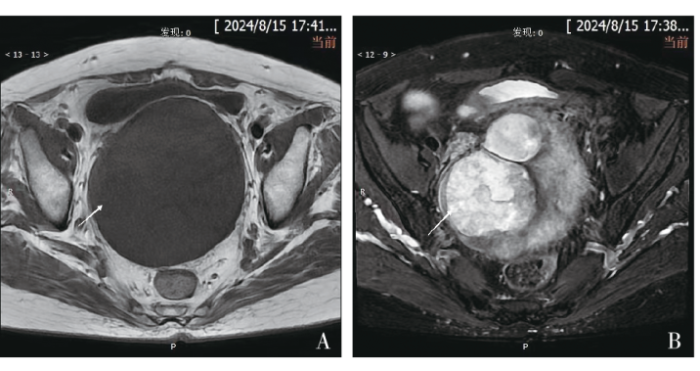
患者为求进一步诊治,排除手术禁忌证后,于2024年9月5日在全身麻醉下行经腹盆腔肿物切除术,术中见:肿物位于盆腔,大小约12 cm×10 cm,肠管及膀胱粘连其上及其周围,固定不动,子宫附件缺如。完整切除盆腔肿物后常规关腹。术中出血多,术中共输注去白细胞悬浮红细胞6 U,冰冻血浆400 mL。术后切除物石蜡病理检查示:(盆腔肿物)梭形细胞肿瘤。免疫组织化学检查示:SMA(-),Desmin(部分+),肌红蛋白(Myoglobin,-),MyoD1(-),成肌蛋白(Myogenin,-),信号转导及转录活化因子6(signal transducer and activator of transcription 6,STAT6,-),雌激素受体(estrogen receptor,ER,部分+),孕激素受体(progesterone receptor,PR,+),钙调蛋白(Calponin,-),Ki-67增殖指数(约3%+)。病理结合免疫组织化学结果,倾向于DAA。患者术后恢复良好,于2024年9月11日顺利出院,随访至2024年11月14日,生存质量良好,现持续随访中。
2 讨论
2.1 流行病学及临床特征
2.2 诊断
2.2.1 影像学检查
DAA发病率较低,临床误诊率极高,因此,特殊的影像学特征对于该病的诊断至关重要。DAA在超声中仅表现为低回声包块,在CT中表现多样,但缺乏特异性,因此其通常只能作为初步筛查手段[6]。而在MRI中DAA可以呈现出清晰的边缘和特征性的漩涡状或分层结构,这有助于与其他肿瘤相鉴别,因此影像学检查中MRI对DAA最具有诊断价值。DAA在MRI图像中,T1WI以低、等信号为主,T2WI表现为高信号或较高信号,这可能与肿瘤中富含大量胶原纤维和血管结构有关[1,3]。既往研究表明,由于DAA基质疏松,且富含黏液,其在DWI序列中也有特殊表现,即肿块在DWI序列中呈现明显的高信号[7]。本例患者术前进行的妇科超声及盆腔CT检查均未发现有意义的阳性征象,而在盆腔MRI检查中呈现出团片状长T1、长或短T2信号,DWI局部呈高信号,提示可能为DAA。更为重要的是,通过盆腔MRI的影像学评估,不仅明确了病灶的具体大小和浸润范围,还提供了病灶与周围组织的关系,为拟定手术方案、手术方式提供指导。
2.2.2 病理学检查
由于DAA缺乏典型的临床表现和症状,术前诊断具有挑战性。因此,组织病理学在确诊中起着至关重要的作用。DAA为良性的间叶源性肿瘤,组织病理学相比其他肿瘤较为独特。①肉眼观:DAA直径常>10 cm,多无包膜或仅部分包膜,形状多样,可表现为球形、半圆形、索状、哑铃形或不规则形。肿瘤多呈分叶状,质地柔软,边界不清晰,呈浸润性生长。切面呈现半透明、黏液水肿和凝胶状,伴有囊性变和出血区[8]。②镜下观:显微镜下肿瘤呈梭形、星芒状,稀疏分布于黏液样细胞基质中。基质中的血管排列杂乱,管径和管壁厚度不均。较大的血管被多层增生的平滑肌细胞包绕,形成厚壁,周围可见急性或慢性炎症细胞浸润及红细胞外渗[9]。③免疫组织化学检查:DAA患者通常Desmin、SMA、ER、PR阳性,S-100和CD68阴性,Ki-67增殖指数较低。免疫组织化学检查结果支持肿瘤细胞可能来源于间充质细胞,具有成纤维细胞和肌成纤维细胞的特征。Ki-67增殖指数较低,与肿瘤生长缓慢、细胞增殖不活跃的特点相一致[10-11]。本例患者肿瘤组织标本经巨检测量最大径为12 cm,包膜完整,切面灰白色,质软,局部呈结节状。镜检肿瘤细胞呈梭形,间质为黏液样,含大小不等的血管。免疫组织化学检查结果示Desmin(部分+),ER、PR均(+),S-100(-),Ki-67增殖指数(约3%+)。病理表现均符合DAA病理特征,DAA诊断明确。
2.3 治疗与预后
DAA虽为良性肿瘤,但生物学行为常表现出恶性肿瘤的特征,即呈无包膜的胶质状生长,常侵袭周围组织。因此认为手术是DAA的主要治疗方法,但复发是最为普遍的问题。据文献统计,约70%患者在术后3年内复发[12]。欧洲一项涉及36例病例的多中心回顾性研究指出,DAA的局部复发率为50%,完全切除后中位复发时间为39个月[13]。因此局部肿物的充分切除并达到切缘阴性是最根本的治疗方法,也是预防肿瘤复发最有效的手段。但由于DAA的侵袭性,临床中术者通常无法明确肿瘤边界,因此选择广泛性切除的手术方式显得尤为重要[14]。但对于浸润深度较深或位于膀胱、直肠等部位的肿瘤,广泛性切除可能会引起严重的术后并发症,影响患者生存质量。因此,Qu等[1]就降低手术风险提出以下建议:①术前进行MRI检查,评估病变范围和邻近器官的浸润程度;②术前根据患者病情应用促性腺激素释放激素(gonadotropin-releasing hormone,GnRH)激动剂或动脉栓塞治疗能够有效降低手术难度、减少损伤,尤其是对于病变深度大于10 cm的患者;③根据病变部位选择合适的手术入路,会阴部浅表或阴道病变宜采用经会阴入路,会阴部组织甚至盆腔深部浸润则需经腹或腹腔镜手术。本例患者高龄,病灶局限于盆腔深部,术前MRI检查未见明显周围组织浸润,故行经腹盆腔肿物切除术完整切除病灶。
但考虑到大多数DAA患者为育龄期女性,为了保护患者的生育力以及提高术后生活质量,有时可以接受部分病灶残留,并在术后辅以内分泌治疗。DAA患者的免疫组织化学检查显示ER、PR阳性,提示该肿瘤可能有激素依赖性。对于绝经后女性,芳香化酶抑制剂较为有效[1,15]。而对于育龄期患者,术后使用GnRH激动剂可能更有助于清除残留病灶,延缓肿瘤复发[12,16]。在Qu等[1]的研究中,术后辅以6个周期的GnRH激动剂治疗未观察到肿瘤复发。但长期使用GnRH激动剂可能会导致绝经期症状,如潮热、盗汗甚至骨质丢失,因此,应根据患者的实际情况选择是否进行激素治疗。本例患者高龄,且手术切缘阴性,因此术后未给予激素辅助治疗。
综上所述,DAA较为罕见,临床表现无特异性,早期诊断困难,一般表现为会阴部逐渐增大的无痛性肿块。因影像学特征特殊,MRI中呈现清晰的边缘和特征性的漩涡状或分层结构时应高度怀疑DAA的可能。手术完整切除病灶是首选的治疗方法,综合评价及预处理会使患者获益更多,术前根据影像学及肿瘤位置选择手术方式,术后个体化治疗,根据患者情况选择是否进行激素治疗,能够更有效地降低肿瘤的复发。DAA虽为良性肿瘤,但具有侵袭性和高复发性,因此建议患者至少进行2年的密切随访,随访内容包括CT、MRI等检查,以便及时发现复发并控制疾病进展。
参考文献
Aggressive angiomyxoma of female pelvis and perineum: Retrospective study of 17 cases
[J].
Aggressive angiomyxoma is an uncommon mesenchymal neoplasm characterized by a high recurrence rate, usually observed in the lower genital tract of women during their reproductive age.Seventeen cases of aggressive angiomyxoma confirmed by pathology from January 2007 to December 2021 in Beijing Chao-yang Hospital were included. We collected clinical data and summarized the clinical and immunohistochemical features.All seventeen included patients were females, aged between 23 and 57 years (mean, 37.7 years; median, 42 years). Fourteen patients were newly diagnosed and three were recurrent. The tumors were located in vulva (58.8 %), vagina (23.5 %), buttock (11.8 %), and cervix (5.9 %). The tumors size were 2 to 15 cm in greatest dimension (mean 8 ± 4.4 cm, median 6 cm). Follow-up data was available for nine patients, which ranged from 25 to 124 months (mean, 82 months; median, 80 months). At the end of follow-up, no other recurrence or metastasis was reported. Immunohistochemical analysis showed immunoreactive for estrogen (10/11) and progesterone (8/11) receptor, desmin (6/8), smooth muscle actin (4/10), and vimentin (4/4), S-100 (1/8) and CD34 (1/7). The Ki67 level was less than 5 % in five cases.AAM is a hormone-sensitive, distinct rare mesenchymal neoplasm with high incidence of local recurrence. Surgery is the preferred treatment, with complete resection being an essential prerequisite for minimizing the risk of recurrence.Copyright © 2024 The Authors. Published by Elsevier B.V. All rights reserved.
Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm
[J].Nine case of a distinctive soft tissue tumor of the female pelvis and perineum are described. They were characterized by their occurrence in young women (ages 21-38), large size (up to 60 X 20 cm), locally infiltrative nature, and grossly gelatinous appearance. The initial clinical impression was usually that of a Bartholin gland cyst. The microscopic appearance was that of spindle or stellate cells widely separated by a loose myxoid stroma focally rich in collagen fibrils, a prominent vascular component, including many large thick-walled vessels without an arborizing pattern, and foci of proliferating glandular elements in two cases. Mitotic activity was exceedingly low. Ultrastructural study of the spindle cells showed features consistent with myofibroblastic differentiation. Four patients developed large local recurrences; one tumor recurred twice, 14 and 15 years after initial excision. No distant metastases have been documented to date, and all patients are alive and well. The differential diagnosis of this unusual tumor includes myxoma, myxoid liposarcoma, sarcoma botryoides, myxoid variant of malignant fibrous histiocytoma, nerve sheath myxoma, and other soft tissue tumors with secondary myxoid changes. We have chosen the term "aggressive angiomyxoma" for this neoplasm to emphasize the neoplastic nature of the blood vessels and its locally infiltrative and recurrent nature.
Aggressive Angiomyxoma of the Pelvis: 35-Year Experience
[J].
双侧坐骨直肠窝侵袭性血管粘液瘤一例
[J].
Aggressive angiomyxoma of perineal
[J].
6例盆腔侵袭性血管粘液瘤影像特征
[J].
侵袭性血管粘液瘤CT、MRI征象及术前评估
[J].
Aggressive angiomyxoma of pelvis: A case report and literature review
[J].
Clinicopathological features and differential diagnosis of aggressive angiomyxoma of the female pelvis: 5 case reports and literature review
[J].
Clinical experiences on aggressive angiomyxoma in China (report of 93 cases)
[J].To discuss the clinical experiences of aggressive angiomyxoma (AAM) by summarizing clinical information of patients with this disease in China.Chinese articles concerning AAM were retrospectively reviewed and analyzed.A total of 93 cases in 44 well-documented articles had been reported, among which 11 were male and 82 were female, with a male to female ratio of 1:7.45. The age of the females varied from 14 to 55 years (mean [SD], 37.17 [10.39] years; median, 38.5 years), whereas that of the males ranged from 15 to 65 years (mean [SD], 44.75 [17.61] years; median, 55 years), which was significantly higher than that of the females (t = 2.082, P = 0.041). The most common sites were the perineum in females and the scrotum in males. None of the cases could be accurately diagnosed as AAM preoperatively. The mean minimum diameter of the tumors was 4.62 (3.51) cm, and the maximum was 9.12 (8.23) cm. All the specimens showed typical pathological features of AAM as reported previously. Immunohistochemistry indicated that AAM tended to be strongly positive for vimentin, smooth-muscle actin, and CD34 but mostly negative for S-100 and CD68. The duration of the postoperative follow-up was 3 to 96 months (mean [SD], 28.5 [18.86] months; median, 9.5 months) in 44 cases, with a recurrence rate of 31.82%.Aggressive angiomyxoma must be considered in the differential diagnosis of any female with an asymptomatic perineal mass. A complete margin-free excision should be achieved to avoid recurrence. Long-term follow-up is quite necessary because of the high rate of local recurrence.
盆腔巨大肿物经脐单孔腹腔镜手术1例并文献复习
[J].
盆底侵袭性血管粘液瘤1例
[J].
Treatment Outcomes and Sensitivity to Hormone Therapy of Aggressive Angiomyxoma: A Multicenter, International, Retrospective Study
[J].
Aggressive Angiomyxoma. A case series of eight years of experience
[J].Aggressive angiomyxoma is a type of mesenchymal tumor occurring predominantly in the pelvic and perineal region. The aim of our study was to reveal our experience with gonadotropin-releasing hormone (GnRH) treatment in patients with angiomyxoma and provide a comprehensive review of management.This study is a case-series including seven female patients diagnosed with aggressive angiomyxoma from a single institution, between 2012 and 2020. Follow-up after surgery was ranged between 2-45 months with an average of 17.6 months. Resection was performed in all patients without any complications, and five had received GnRH analogue (Goserelin acetate) therapy after surgery. Immunohistochemistry analyses showed positivity for smooth muscle actin and desmin in all cases, while both estrogen receptor (ER) and progesterone receptor (PR) positivity were identified in 6 patients. None of the seven patients had recurrence during follow up period.The mean treatment of aggressive angiomyxoma is surgery, and the use of GnHR analogues in cases with positive ER and PR may be effective in preventing recurrence.Aggressive Angiomyxoma, Gonadotropin-Releasing Hormone, Soft Tissue Neoplasm.
外阴侵袭性血管粘液瘤2例
[J].
Aggressive angiomyxoma in pregnancy: a case report and literature review
[J].

{kind=link}
{kind=link}