国际妇产科学杂志 ›› 2026, Vol. 53 ›› Issue (1): 85-88.doi: 10.12280/gjfckx.20251335
吕寒雪( ), 徐金颖, 刘华()
), 徐金颖, 刘华()
LYU Han-xue(), XU Jin-ying, LIU Hua()
摘要:
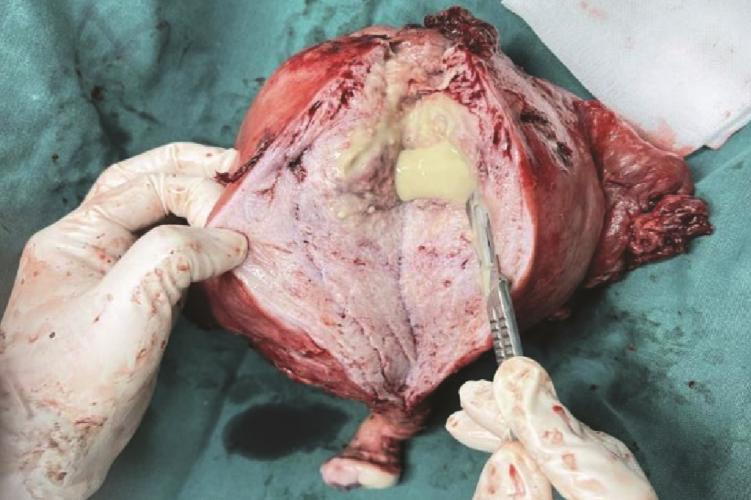
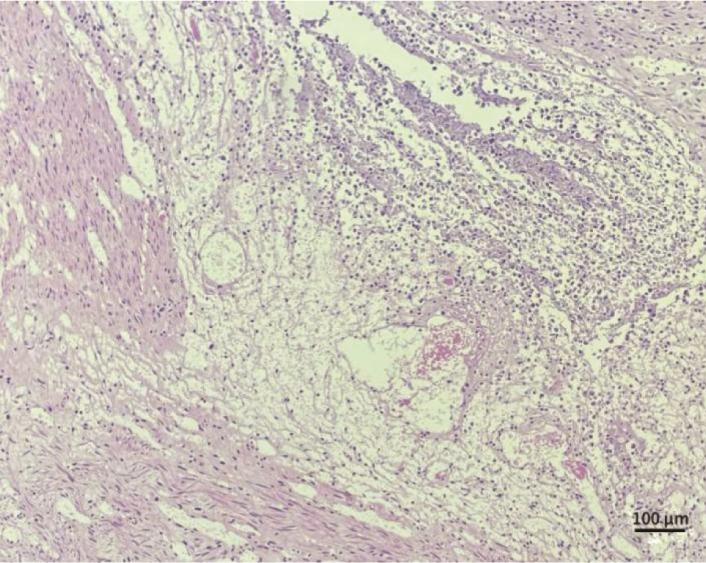
报告1例50岁子宫腺肌病合并子宫肌壁间脓肿及输卵管积脓患者。患者因腹痛、发热入院,检查提示重症感染(白细胞47.05×109/L)及子宫显著增大。初始经验性抗生素(亚胺培南西司他丁钠)治疗后感染指标部分下降,但腹痛加剧并出现腹腔积液,怀疑脓肿破裂。急行经腹全子宫切除术+双侧附件切除术+盆腔粘连松解术+肠粘连分解术,术中见盆腔脓性分泌物,术后剖视子宫标本证实肌壁间存在多发脓腔,病理诊断符合子宫腺肌瘤伴感染及脓肿形成。术后根据病原学结果继续抗感染及支持治疗,患者感染得到控制。本例提示子宫腺肌病可能成为盆腔感染扩散、形成深部肌壁间脓肿的基础。对于此类复杂性感染,在强效抗生素治疗下若病情反复或疑有脓肿破裂,采取手术治疗控制感染源是成功救治的关键。