Journal of International Obstetrics and Gynecology ›› 2024, Vol. 51 ›› Issue (1): 21-27.doi: 10.12280/gjfckx.20230728
• Obstetric Physiology & Obstetric Disease: Original Article • Previous Articles Next Articles
ZHANG Ting, CHEN Zhen-yu( ), LIU Sen, ZHANG Xiao-hong, LI Ya-meng, LI Cai-xi
), LIU Sen, ZHANG Xiao-hong, LI Ya-meng, LI Cai-xi
Received:2023-09-15
Published:2024-02-15
Online:2024-02-19
Contact:
CHEN Zhen-yu
E-mail:czy740704@163.com
ZHANG Ting, CHEN Zhen-yu, LIU Sen, ZHANG Xiao-hong, LI Ya-meng, LI Cai-xi. Construction and Validation of A Predictive Model for Adverse Pregnancy Outcomes in Preeclampsia[J]. Journal of International Obstetrics and Gynecology, 2024, 51(1): 21-27.
Add to citation manager EndNote|Ris|BibTeX
| 变量 | 不良结局组 (n=289) | 无不良结局组 (n=450) | χ2 | P |
|---|---|---|---|---|
| 高龄(≥35岁) | 64(22.15) | 91(20.22) | 0.393 | 0.531 |
| 妊娠前BMI(kg/m2) | 9.246 | 0.026 | ||
| ≤18.5 | 22(7.61) | 37(8.22) | ||
| 18.5~<25 | 135(46.71) | 256(56.89) | ||
| 25~<28 | 67(23.18) | 86(19.11) | ||
| ≥28 | 65(22.49) | 71(15.78) | ||
| 初产妇 | 231(79.93) | 355(78.89) | 0.116 | 0.733 |
| 辅助生殖技术妊娠 | 48(16.61) | 36(8.0) | 12.946 | <0.001 |
| 流产史 | 86(29.76) | 134(29.78) | 0.000 | 0.995 |
| 多胎妊娠 | 11(3.81) | 17(3.78) | 0.000 | 0.984 |
| 妊娠前糖尿病 | 21(7.27) | 20(4.44) | 2.674 | 0.102 |
| 妊娠期高血压病史 | 11(3.81) | 9(2.00) | 2.180 | 0.140 |
| 子痫前期病史 | 8(2.77) | 2(0.44) | 5.484 | 0.019 |
| 合并妊娠期糖尿病 | 52(17.99) | 91(20.22) | 0.560 | 0.454 |
| 合并妊娠期甲减 | 29(10.03) | 56(12.44) | 1.004 | 0.316 |
| 合并免疫系统疾病 | 3(1.04) | 6(1.33) | 0.000 | 0.989 |
| 收缩压≥160 mmHg | 107(37.02) | 69(15.33) | 45.634 | <0.001 |
| 舒张压≥110 mmHg | 76(26.30) | 40(8.89) | 40.303 | <0.001 |
| 平均动脉压≥120 mmHg | 128(44.29) | 88(19.56) | 52.051 | <0.001 |
| 浆膜腔积液 | 40(13.84) | 40(8.89) | 4.470 | 0.034 |
| 脐血流异常 | 119(41.18) | 105(23.33) | 26.524 | <0.001 |
| 发病孕周(周) | 109.195 | <0.001 | ||
| ≥37 | 78(26.99) | 239(53.11) | ||
| 34~<37 | 30(10.38) | 95(21.11) | ||
| 32~≤34 | 71(24.57) | 67(14.89) | ||
| ≤32 | 110(38.06) | 49(10.89) | ||
| FGR | 131(45.33) | 25(5.56) | 167.164 | <0.001 |
| 临床症状 | ||||
| 腹痛 | 30(10.38) | 28(6.22) | 4.208 | 0.040 |
| 头晕/头痛 | 32(11.07) | 27(6.00) | 6.164 | 0.013 |
| 恶心/呕吐 | 3(1.04) | 5(1.11) | 0.000 | 1.000 |
| 胸闷/呼吸困难 | 5(1.73) | 2(0.44) | 1.881 | 0.170 |
| 视物模糊/视觉障碍 | 11(3.81) | 13(2.89) | 0.471 | 0.492 |
| 临床症状数量(个)* | 11.270 | 0.004 | ||
| 0 | 219(75.78) | 385(85.56) | ||
| 1 | 59(20.42) | 55(12.22) | ||
| ≥2 | 11(3.81) | 10(2.22) | ||
| FIB≤4 g/L | 148(51.21) | 75(16.67) | 99.668 | <0.001 |
| PLT≤100×109/L | 65(22.49) | 18(4.00) | 60.355 | <0.001 |
| Hb<110 g/L | 119(26.44) | 74(25.61) | 0.064 | 0.800 |
| ALT≥40 U/L | 16(5.54) | 10(2.22) | 5.694 | 0.017 |
| AST≥35 U/L | 34(11.76) | 32(7.11) | 4.686 | 0.030 |
| ALB≤30 g/L | 150(51.90) | 97(21.56) | 72.835 | <0.001 |
| 尿蛋白定性 | 178.840 | <0.001 | ||
| + | 49(16.96) | 279(62.00) | ||
| ++ | 108(37.37) | 126(28.0) | ||
| +++~++++ | 132(45.67) | 45(10.00) | ||
| Cr≥73 μmol/L | 36(12.46) | 54(12.00) | 0.034 | 0.853 |
| UA≥410 μmol/L | 64(22.51) | 124(27.56) | 2.716 | 0.099 |
| LDH≥263 U/L | 191(66.09) | 72(16.0) | 192.617 | <0.001 |
| 变量 | 不良结局组 (n=289) | 无不良结局组 (n=450) | χ2 | P |
|---|---|---|---|---|
| 高龄(≥35岁) | 64(22.15) | 91(20.22) | 0.393 | 0.531 |
| 妊娠前BMI(kg/m2) | 9.246 | 0.026 | ||
| ≤18.5 | 22(7.61) | 37(8.22) | ||
| 18.5~<25 | 135(46.71) | 256(56.89) | ||
| 25~<28 | 67(23.18) | 86(19.11) | ||
| ≥28 | 65(22.49) | 71(15.78) | ||
| 初产妇 | 231(79.93) | 355(78.89) | 0.116 | 0.733 |
| 辅助生殖技术妊娠 | 48(16.61) | 36(8.0) | 12.946 | <0.001 |
| 流产史 | 86(29.76) | 134(29.78) | 0.000 | 0.995 |
| 多胎妊娠 | 11(3.81) | 17(3.78) | 0.000 | 0.984 |
| 妊娠前糖尿病 | 21(7.27) | 20(4.44) | 2.674 | 0.102 |
| 妊娠期高血压病史 | 11(3.81) | 9(2.00) | 2.180 | 0.140 |
| 子痫前期病史 | 8(2.77) | 2(0.44) | 5.484 | 0.019 |
| 合并妊娠期糖尿病 | 52(17.99) | 91(20.22) | 0.560 | 0.454 |
| 合并妊娠期甲减 | 29(10.03) | 56(12.44) | 1.004 | 0.316 |
| 合并免疫系统疾病 | 3(1.04) | 6(1.33) | 0.000 | 0.989 |
| 收缩压≥160 mmHg | 107(37.02) | 69(15.33) | 45.634 | <0.001 |
| 舒张压≥110 mmHg | 76(26.30) | 40(8.89) | 40.303 | <0.001 |
| 平均动脉压≥120 mmHg | 128(44.29) | 88(19.56) | 52.051 | <0.001 |
| 浆膜腔积液 | 40(13.84) | 40(8.89) | 4.470 | 0.034 |
| 脐血流异常 | 119(41.18) | 105(23.33) | 26.524 | <0.001 |
| 发病孕周(周) | 109.195 | <0.001 | ||
| ≥37 | 78(26.99) | 239(53.11) | ||
| 34~<37 | 30(10.38) | 95(21.11) | ||
| 32~≤34 | 71(24.57) | 67(14.89) | ||
| ≤32 | 110(38.06) | 49(10.89) | ||
| FGR | 131(45.33) | 25(5.56) | 167.164 | <0.001 |
| 临床症状 | ||||
| 腹痛 | 30(10.38) | 28(6.22) | 4.208 | 0.040 |
| 头晕/头痛 | 32(11.07) | 27(6.00) | 6.164 | 0.013 |
| 恶心/呕吐 | 3(1.04) | 5(1.11) | 0.000 | 1.000 |
| 胸闷/呼吸困难 | 5(1.73) | 2(0.44) | 1.881 | 0.170 |
| 视物模糊/视觉障碍 | 11(3.81) | 13(2.89) | 0.471 | 0.492 |
| 临床症状数量(个)* | 11.270 | 0.004 | ||
| 0 | 219(75.78) | 385(85.56) | ||
| 1 | 59(20.42) | 55(12.22) | ||
| ≥2 | 11(3.81) | 10(2.22) | ||
| FIB≤4 g/L | 148(51.21) | 75(16.67) | 99.668 | <0.001 |
| PLT≤100×109/L | 65(22.49) | 18(4.00) | 60.355 | <0.001 |
| Hb<110 g/L | 119(26.44) | 74(25.61) | 0.064 | 0.800 |
| ALT≥40 U/L | 16(5.54) | 10(2.22) | 5.694 | 0.017 |
| AST≥35 U/L | 34(11.76) | 32(7.11) | 4.686 | 0.030 |
| ALB≤30 g/L | 150(51.90) | 97(21.56) | 72.835 | <0.001 |
| 尿蛋白定性 | 178.840 | <0.001 | ||
| + | 49(16.96) | 279(62.00) | ||
| ++ | 108(37.37) | 126(28.0) | ||
| +++~++++ | 132(45.67) | 45(10.00) | ||
| Cr≥73 μmol/L | 36(12.46) | 54(12.00) | 0.034 | 0.853 |
| UA≥410 μmol/L | 64(22.51) | 124(27.56) | 2.716 | 0.099 |
| LDH≥263 U/L | 191(66.09) | 72(16.0) | 192.617 | <0.001 |
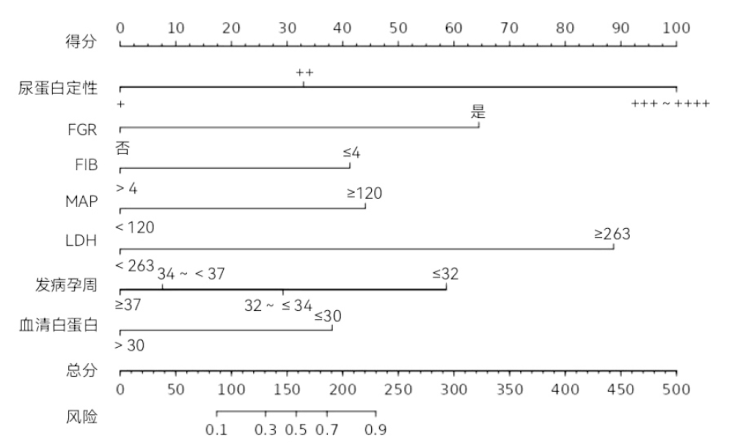
| 因素 | B | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 发病孕周 | |||||
| ≥37周 | - | - | - | - | - |
| 34~<37周 | 0.25 | 0.41 | 0.36 | 0.548 | 1.28(0.57~2.85) |
| 32~≤34周 | 0.95 | 0.39 | 6.02 | 0.014 | 2.58(1.21~5.49) |
| ≤32周 | 1.85 | 0.39 | 22.91 | <0.001 | 6.33(2.97~13.49) |
| 平均动脉压≥120 mmHg | 1.25 | 0.38 | 10.88 | 0.001 | 3.47(1.66~7.27) |
| FGR | 1.84 | 0.41 | 19.78 | <0.001 | 6.28(2.79~14.13) |
| FIB≤4 g/L | 1.29 | 0.29 | 20.77 | <0.001 | 3.66(2.09~6.40) |
| 尿蛋白定性 | |||||
| + | - | - | - | - | - |
| ++ | 1.01 | 0.29 | 11.79 | 0.001 | 2.76(1.55~4.91) |
| +++~++++ | 3.06 | 0.38 | 65.10 | <0.001 | 21.26(10.12~44.68) |
| ALB≤30 g/L | 1.21 | 0.29 | 17.56 | <0.001 | 3.34(1.90~5.88) |
| LDH≥263 U/L | 2.81 | 0.29 | 92.37 | <0.001 | 16.59(9.36~29.43) |
| 常量 | -5.12 | 0.42 | 146.83 | 0.000 | 0.006 |
| 因素 | B | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 发病孕周 | |||||
| ≥37周 | - | - | - | - | - |
| 34~<37周 | 0.25 | 0.41 | 0.36 | 0.548 | 1.28(0.57~2.85) |
| 32~≤34周 | 0.95 | 0.39 | 6.02 | 0.014 | 2.58(1.21~5.49) |
| ≤32周 | 1.85 | 0.39 | 22.91 | <0.001 | 6.33(2.97~13.49) |
| 平均动脉压≥120 mmHg | 1.25 | 0.38 | 10.88 | 0.001 | 3.47(1.66~7.27) |
| FGR | 1.84 | 0.41 | 19.78 | <0.001 | 6.28(2.79~14.13) |
| FIB≤4 g/L | 1.29 | 0.29 | 20.77 | <0.001 | 3.66(2.09~6.40) |
| 尿蛋白定性 | |||||
| + | - | - | - | - | - |
| ++ | 1.01 | 0.29 | 11.79 | 0.001 | 2.76(1.55~4.91) |
| +++~++++ | 3.06 | 0.38 | 65.10 | <0.001 | 21.26(10.12~44.68) |
| ALB≤30 g/L | 1.21 | 0.29 | 17.56 | <0.001 | 3.34(1.90~5.88) |
| LDH≥263 U/L | 2.81 | 0.29 | 92.37 | <0.001 | 16.59(9.36~29.43) |
| 常量 | -5.12 | 0.42 | 146.83 | 0.000 | 0.006 |
| 实际结局 | 预测结局 | 合计 | |
|---|---|---|---|
| 不良妊娠结局 | 无不良妊娠结局 | ||
| 不良妊娠结局 | 37 | 9 | 46 |
| 无不良妊娠结局 | 8 | 71 | 79 |
| 合计 | 45 | 80 | 125 |
| 实际结局 | 预测结局 | 合计 | |
|---|---|---|---|
| 不良妊娠结局 | 无不良妊娠结局 | ||
| 不良妊娠结局 | 37 | 9 | 46 |
| 无不良妊娠结局 | 8 | 71 | 79 |
| 合计 | 45 | 80 | 125 |
| [1] |
Brown MA, Magee LA, Kenny LC, et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice[J]. Hypertension, 2018, 72(1):24-43. doi: 10.1161/HYPERTENSIONAHA.117.10803.
pmid: 29899139 |
| [2] | 国家卫生健康委员会. 中国健康卫生统计年鉴(2022)[M]. 北京: 中国协和医科大学出版社, 2022:220-221. |
| [3] |
Li F, Qin J, Zhang S, et al. Prevalence of hypertensive disorders in pregnancy in China: A systematic review and meta-analysis[J]. Pregnancy Hypertens, 2021, 24:13-21. doi: 10.1016/j.preghy.2021.02.001.
pmid: 33626437 |
| [4] | Ma'ayeh M, Costantine MM. Prevention of preeclampsia[J]. Semin Fetal Neonatal Med, 2020, 25(5):101123. doi: 10.1016/j.siny.2020.101123. |
| [5] | von Dadelszen P, Payne B, Li J, et al. Prediction of adverse maternal outcomes in pre-eclampsia: development and validation of the fullPIERS model[J]. Lancet, 2011,377(9761):219-227. doi: 10.1016/ S0140-6736(10)61351-7. |
| [6] |
Escobar GJ, Soltesz L, Schuler A, et al. Prediction of obstetrical and fetal complications using automated electronic health record data[J]. Am J Obstet Gynecol, 2021, 224(2):137-147.e7. doi: 10.1016/j.ajog.2020.10.030.
pmid: 33098815 |
| [7] | Saleh L, Alblas MM, Nieboer D, et al. Prediction of pre-eclampsia-related complications in women with suspected or confirmed pre-eclampsia: development and internal validation of clinical prediction model[J]. Ultrasound Obstet Gynecol, 2021, 58(5):698-704. doi: 10.1002/uog.23142. |
| [8] |
Tan J, Yang M, Liao Y, et al. Development and validation of a prediction model on severe maternal outcomes among pregnant women with pre-eclampsia: a 10-year cohort study[J]. Sci Rep, 2020, 10(1):15590. doi: 10.1038/s41598-020-72527-0.
pmid: 32973289 |
| [9] | 廖媛, 刘兴会, 谭婧, 等. 建立子痫前期不良结局风险预警模型的初步研究[J]. 四川大学学报(医学版), 2018, 49(5):797-802. |
| [10] | 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2020)[J]. 中华妇产科杂志, 2020, 55(4):227-238. doi: 10.3760/cma.j.cn112141-20200114-00039. |
| [11] | American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics and the Society for Maternal-Fetal Medicine. ACOG Practice Bulletin No. 204: Fetal Growth Restriction[J]. Obstet Gynecol, 2019, 133(2):e97-e109. doi: 10.1097/AOG.0000000000003070. |
| [12] |
Bakrania BA, Spradley FT, Drummond HA, et al. Preeclampsia: Linking Placental Ischemia with Maternal Endothelial and Vascular Dysfunction[J]. Compr Physiol, 2020, 11(1):1315-1349. doi: 10.1002/cphy.c200008.
pmid: 33295016 |
| [13] | McCracken SA, Seeho S, Carrodus T, et al. Dysregulation of Oxygen Sensing/Response Pathways in Pregnancies Complicated by Idiopathic Intrauterine Growth Restriction and Early-Onset Preeclampsia[J]. Int J Mol Sci, 2022, 23(5):2772. doi: 10.3390/ijms23052772. |
| [14] | Willy D, Willy K, Köster HA, et al. Blood Pressure Levels and Maternal Outcome in Women with Preeclampsia - a Retrospective Study from a Large Tertiary Obstetric Centre[J]. Geburtshilfe Frauenheilkd, 2022, 82(5):528-534. doi: 10.1055/a-1783-7718. |
| [15] | Balogun OA, Khangura RK, Kregel HR, et al. Erratum: Preterm Preeclampsia with Severe Features: Composite Maternal and Neonatal Morbidities Associated with Fetal Growth Restriction[J]. Am J Perinatol, 2018, 35(8):e2. doi: 10.1055/s-0039-1697912. |
| [16] | 陈娟娟, 孙雯, 苏春宏, 等. 子痫前期并发胎儿生长受限的临床特征及妊娠结局分析[J]. 中华产科急救电子杂志, 2021, 10(2):89-95. doi: 10.3877/cma.j.issn.2095-3259.2021.02.006. |
| [17] |
Obata S, Toda M, Tochio A, et al. Fetal growth restriction as a diagnostic criterion for preeclampsia[J]. Pregnancy Hypertens, 2020, 21:58-62. doi: 10.1016/j.preghy.2020.05.002.
pmid: 32413588 |
| [18] | Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222[J]. Obstet Gynecol, 2020, 135(6):e237-e260. doi: 10.1097/AOG.0000000000003891. |
| [19] | Lei T, Qiu T, Liao W, et al. Proteinuria may be an indicator of adverse pregnancy outcomes in patients with preeclampsia: a retrospective study[J]. Reprod Biol Endocrinol, 2021, 19(1):71. doi: 10.1186/s12958-021-00751-y. |
| [20] |
Morikawa M, Mayama M, Saito Y, et al. Hypoproteinemia as a parameter of poor perinatal/neonatal outcomes in women with preeclampsia diagnosed as hypertension plus proteinuria[J]. Pregnancy Hypertens, 2020, 21:111-117. doi: 10.1016/j.preghy.2020.05.012.
pmid: 32492636 |
| [21] | 王晓旭, 刘俊涛, 高劲松, 等. 尿蛋白水平对于评估子痫前期严重程度及母儿结局的价值[J]. 中华妇产科杂志, 2022, 57(5):325-331. doi: 10.3760/cma.j.cn112141-20211103-00641. |
| [22] | Tochio A, Obata S, Saigusa Y, et al. Does pre-eclampsia without proteinuria lead to different pregnancy outcomes than pre-eclampsia with proteinuria?[J]. J Obstet Gynaecol Res, 2019, 45(8):1576-1583. doi: 10.1111/jog.14017. |
| [23] | Khidri FF, Shaikh F, Khowaja IU, et al. Role of Lactate Dehydrogenase in the Prediction of Severity in Pre-Eclampsia[J]. Curr Hypertens Rev, 2020, 16(3):223-228. doi: 10.2174/1573402116666200720001032. |
| [24] |
Guida JP, Cralcev C, Costa Santos J, et al. Validation of the fullPIERS model for prediction of adverse outcomes in preeclampsia at a referral center[J]. Pregnancy Hypertens, 2021, 23:112-115. doi: 10.1016/j.preghy.2020.11.013.
pmid: 33310390 |
| [25] |
Almeida ST, Katz L, Coutinho I, et al. Validation of fullPIERS model for prediction of adverse outcomes among women with severe pre-eclampsia[J]. Int J Gynaecol Obstet, 2017, 138(2):142-147. doi: 10.1002/ijgo.12197.
pmid: 28475234 |
| [26] | 沈敏红, 韩冰. fullPIERS预测模型用于574例妊娠高血压人群的初探[J]. 现代妇产科进展, 2012, 21(3):172-174,178. |
| [27] |
Dröge LA, Perschel FH, Stütz N, et al. Prediction of Preeclampsia-Related Adverse Outcomes With the sFlt-1 (Soluble fms-Like Tyrosine Kinase 1)/PlGF (Placental Growth Factor)-Ratio in the Clinical Routine: A Real-World Study[J]. Hypertension, 2021, 77(2):461-471. doi: 10.1161/HYPERTENSIONAHA.120.15146.
pmid: 33280406 |
| [1] | MA Ling, LI Ya-xi, ZHAO Min, WANG Jing, LI Hong-li. Progress on the Relationship between Apoptosis and Adverse Pregnancy Outcomes [J]. Journal of International Obstetrics and Gynecology, 2025, 52(2): 121-126. |
| [2] | YANG Yang, MA Yuan, CHEN You-yi, ZHAO Jing, MA Wen-juan. The Effect of Serum Exosomes from Patients with Severe Preeclampsia on the Function of Normal Decidual Immune Cells in Humans [J]. Journal of International Obstetrics and Gynecology, 2025, 52(2): 143-152. |
| [3] | GENG Hao, CHEN Xu. The Characteristics of Premature Labor and Intrapartum Management [J]. Journal of International Obstetrics and Gynecology, 2025, 52(1): 105-109. |
| [4] | WANG Jing, WANG Yong-hong. Decidual Natural Killer Cells in the Pathogenesis of Preeclampsia: A Review [J]. Journal of International Obstetrics and Gynecology, 2025, 52(1): 88-93. |
| [5] | ZHANG Wen, LIU Hui-qiang. The Role of SOCS1 and Exosomal MicroRNA in the Pathogenesis of Preeclampsia [J]. Journal of International Obstetrics and Gynecology, 2025, 52(1): 94-98. |
| [6] | WANG Yi-dan, WANG Yong-hong. The Role of the Transforming Growth Factor-β Superfamily in the Pathogenesis of Preeclampsia [J]. Journal of International Obstetrics and Gynecology, 2025, 52(1): 99-104. |
| [7] | FAN Bo-yang, HU Li-yan. Research Advancements on the Pathogenesis and Prediction Approaches of Twin Pregnancies Complicated with Preeclampsia [J]. Journal of International Obstetrics and Gynecology, 2024, 51(6): 611-615. |
| [8] | MA Guo-xia, WANG Jia-li, MIAO He-zhen, YAN Yu, LIU Jia-jia, YANG Yong-xiu. Pregnancy Complicated with Ebstein Anomaly: Two Cases Report [J]. Journal of International Obstetrics and Gynecology, 2024, 51(6): 624-628. |
| [9] | DENG Ling-ling, WU Shao-wen, ZHANG Wei-yuan. Research Progress on Low-Dose Aspirin in the Prevention of Preeclampsia [J]. Journal of International Obstetrics and Gynecology, 2024, 51(5): 515-518. |
| [10] | TANG Shi-cheng, ZHANG Guo-ying. Effects of Intraspinal Labor Analgesia on Maternal and Neonatal Outcomes [J]. Journal of International Obstetrics and Gynecology, 2024, 51(5): 519-524. |
| [11] | ZHANG Qi, WANG Xin, REN Yi, LIU Chao, GAO Hui-jie. Research Progress on SLRPs in Placental Development and Pregnancy-Related Diseases [J]. Journal of International Obstetrics and Gynecology, 2024, 51(5): 525-530. |
| [12] | ZHANG Yong-qing, CHEN Dan-qing, CHEN Lu-ping, MA Xin-rui, CAI Wang-ying, WANG Mei-lin. The Value of Early Pregnancy Fasting Serum ANGPTL-2 and ANGPTL-8 Levels in Predicting Gestational Diabetes Mellitus Based on Propensity Score Matching [J]. Journal of International Obstetrics and Gynecology, 2024, 51(5): 536-540. |
| [13] | LIU Zhao, ZHAO Lin-lin, LI Xia, WANG Xi-xian. Study on the Interaction and Predictive Value of Early Pregnancy BMI and 25-(OH)D3 in Gestational Diabetes Mellitus [J]. Journal of International Obstetrics and Gynecology, 2024, 51(5): 541-545. |
| [14] | REN Yi, HU Yu-lian, WANG Xin, ZHANG Qi, LIU Chao, GAO Hui-jie. Clinical Application and Modern Pharmacological Progress of Traditional Chinese Medicine in Preeclampsia [J]. Journal of International Obstetrics and Gynecology, 2024, 51(4): 442-447. |
| [15] | ZHAO Li-xia, WANG Xiao-qing. Confused Problem of Magnesium Sulfate in the Treatment of Preeclampsia and Its Adverse Effects [J]. Journal of International Obstetrics and Gynecology, 2024, 51(4): 448-452. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||